by Andrea | Jul 29, 2012
I don’t often think about my life in terms of percentages, particularly as a way of judging success, but there are times when it is hard to avoid. For example, as sub-interns (the fancy word for fourth year medical students on more intensive rotations, such as in the ICU), we are expected to have off one day in every seven, or a total of four for the rotation. If a normal workweek, one in which the weekend is free, is 5/7, or 71.4%, then my workweek is 6/7, or 85.7%. This leaves only 14.3% of my time as free, which is small. Smaller even than the proportion of arterial lines that I have successfully placed, which is what prompted the writing of this post. An arterial line, or art line, or a-line as you may hear, dear readers, is a special IV that goes into an artery, most often the radial artery in the wrist. It allows for the easy drawing of arterial blood for labs, for continuous blood pressure monitoring, and for the humiliation of every medical student who ever did an ICU rotation. I have attempted the placement of five arterial lines, six if you count the one that I missed the first time but then got later after the one my resident placed failed, and that I subsequently got, as two separate lines. I have successfully placed two. That’s right, two. That gives me a resounding 33% or 40% success rate, depending on the counting I mentioned above. This is not reassuring. It is, however, profoundly humbling, which is probably not a bad thing. Maybe humility is what the ICU teaches most effectively of all?
by Andrea | Jul 18, 2012
I know the title sounds approximately as riveting as not at all, but I’ve been thinking a lot about it since I’ve started my ICU month. While I’ve been reflecting on the medical decisions I’m making, in the time I take to process everything I’ve seen, I’ve been focused more on those we expect the patients and families we care for to make. We call on them during their most dire hours and ask them to consider options they don’t necessarily understand, to weigh risks and benefits that are hard to put into context, and to make calls that no one ever wants to have to make. And they do it. Not always with the calm and rational process that would be easiest for the physicians working for them, but more often than not with an incredible degree of grace and reflection mixed into the grief and frustration.
The conversations are almost always accompanied by a great deal of sighing, sobbing, and shouting, which can be disconcerting to those of us working to provide medical care. I think what made me most frustrated back when President Obama’s plans to encourage the discussion of advanced directives turned into a death panel debacle, was the callousness of it with regard to the families of critically ill patients. How many of the individuals who were most loudly heard during that national discussion had been in the position of trying to determine the appropriate goals of care for a loved one at the end of life? I’d hazard a guess that there were very few. Anyone who has had to weigh these questions, particularly without the benefit of a signed document crafted by the patient him/herself charging the course ahead, would think twice about protesting a more considered approach.
With or without a mandate from the government, however, I increasingly believe that physicians and other healthcare providers have a serious obligation to discuss end of life care with all of their patients. A few questions about code status when a person is hospitalized (i.e., whether or not an individual would want chest compressions, shocks to the heart, or other measures to bring back a patient whose heart has stopped while in the hospital) are simply not enough. Although I have been impressed with the way many of my teachers and mentors have navigated these challenging situations with hospitalized patients and their loved ones, I can’t help but wish that as a nation we could pause, reflect on what we want from our last weeks, days, and hours, and take a moment to write it down.
Looking for more resources on Advanced Directives and Living Wills? Check here for the UMHS Publication.
by Andrea | Jun 19, 2012
As has been discussed here previously, I’m training for a large bike ride that is coming up in less than a month. As usual, I’ve been tracking not only my mileage and speed, but also my ranking on BikeJournal. I like to think of it as my keeping-up-with-the-crazy-cycling-Jones-o-meter. If I’m rising in the ranks, then I’m biking more than the average member, and if I’m falling, I’m not keeping up. Granted, in order to stay even one really only needs to bike about 2 miles per day, but it’s still an interesting metric, and plotting it over time makes it even more interesting.
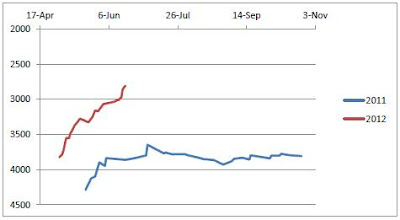


Look how much awesomer I am than last year! So far my predictions about dermatology and research rotations as good for biking are bearing out. Check back in another month or so to see what kind of curve the ICU month generates…
My training schedule marches ever onward, and I’ve been looking for longer rides to fit into my training schedule. Luckily, I received a copy of Cycling Michigan: 30 of the Best Bike Routes in East Michigan by Karen Gentry for either my birthday or Christmas over the winter, and stuck it on my shelf for summer reference. I pulled it out a few weeks ago and was pleasantly surprised! It features lots of rides, as the title suggests, in the eastern part of our lovely state, and includes quite a few that start in or near Ann Arbor. Because Michigan has so many beautiful places to ride, it can be hard to find a book with more than one ride in any given place, but Ms. Gentry does not disappoint.

The first ride from the book took us through some beautiful countryside out to Manchester and back. Here is my bike posing for the picture.
My one complaint about the book is that each ride is described in copious detail without a succinct cue sheet or list of turns, and the maps are not detailed enough to use alone. On the first ride I did from the book, I simply copied the pages describing the ride and stuffed them into my jersey pocket. I had to stop frequently to read through the text to figure out where I should turn next. Two weeks later, much the wiser, I went through the book before the ride, typing up a cue sheet and copying the map onto the lower half. It was much easier to just follow the turns and glance at the map for reassurance. I love the routes in the book, but would recommend a little prep work to make for a better ride!
 The second ride went through Dexter, Pinckney, Brighton, and yes, Hell, MI.
The second ride went through Dexter, Pinckney, Brighton, and yes, Hell, MI.
Another thing that makes for a better ride: doughnuts! I could not write a post about my recent bike rides without mentioning the Dexter Bakery. They make by far the finest apple fritter I have ever consumed, as well as wonderful soft pretzles and regular doughnuts as well; I would highly recommend it as a cycling stop. It’s conveniently located about 11 miles from downtown Ann Arbor, making it an imminently reasonable cycling destination. Yum!
by Andrea | May 17, 2012
I learned a lot last year, and one of the oft repeated nuggets of wisdom shared by residents and more advanced students alike was the joy of the year to come. They promised a less intense grading environment, electives chosen for purposes other than fulfilling core requirements, and more free nights and weekends. So far this is mostly true. I’m in the midst of a dermatology rotation at Henry Ford, a community teaching hospital in Detroit that is connected most closely to Wayne state, but at which UM students have the opportunity to do a few M4 year rotations. In spite of the fact that everyone seems slightly horrified that I’m not planning to go into dermatology, I’ve gotten to see a wide variety of dermatologic complaints while working with delightful residents and attending physicians.
Lessons I’ve already been applying from M3 year:
- You will never know exactly where you should be or what you should do, so don’t be afraid to ask questions.
- Smile a lot. People are less likely to think you are dumb if you also appear friendly and they like you.
- Fake it. Listen closely to what your resident asks of patients so that when you have to see a patient by yourself, you know what questions they will think are important to ask and report back. Eventually you will make it and understand why they have asked those questions.
- Wear gloves. Especially when someone has a rash on the palms of their hands, as it could be secondary syphilis and that is contagious through the rash.
New lessons I’m already learning about M4 year:
- The word elective not only means something you chose, but also something that is not required of everyone. This means that the rest of your medical school training is unlikely to have covered this material and you will need to read a lot.
- When someone tells you that something will be the best “X” since kindergarten, they do not necessarily mean that the entire thing will be filled with naps and snacks. They might mean that you can pick your poisons and that your schedule will be more predictable than previously.
- Smile more. Especially when someone gives you the stink eye after you delicately explain that you are leaning strongly toward (read: have already chosen) another specialty and are just there to learn about their specialty, not to audition for their residency program.
by Andrea | May 5, 2012
Or, thinking about the residency application process
Right before I finished my last rotation of M3 year, I had the opportunity to attend a dinner hosted by the Department of Obstetrics and Gynecology for prospective residency applicants. It was a great chance to say hello again to the residents and faculty I worked with on my rotation and to learn a bit more about the application process. These sorts of events are often overwhelming and sometimes cryptic, but I was particularly struck by the reassurances from many of the faculty.
“Come talk to us, we will help you make a list that will work for you.”
“People who come and talk to us are happy with their matches. We can help you identify the right programs.”
“No, there isn’t another way to find good programs. Come talk to us.”
I left feeling like there was a sorting hat that would sit on my head, discern my clinical grades and Step 1 score, geographical and program-type preferences, and spit out a list of 15-20 programs to which I should apply. While this seems a little fantastic, it is closer to true than you might imagine. Having met now with three faculty members to talk about this process, I’ve come away with three fairly comprehensive lists of programs to consider.
For those of you not already familiar with this process (and those of you who are can skip to the next paragraph), the residency selection process is a match. Students submit applications through a central application system, and much like many other application processes, schools that are interested in particular candidates can offer them interviews. The similarity with most systems stops there, however. After the interviews, each applicant makes a rank list of programs and each program makes a rank list of applicants. These lists are fed to a computer algorithm that matches applicants and programs. The result it spits out is legally binding for one year. Because of this process, the list of program list an applicants starts with is important – there is only one application/interview cycle so there is no (easy*) way to go back and apply if one’s rank list seems a little thin or the match doesn’t go well.
As I’m looking over all of my lists, I’m wishing that there really were a sorting hat that could spit out a definitive set of options, but there aren’t, and honestly, I feel pretty lucky just to have a good sense of what specialty I’m entering and what I’m looking for in a program. I’ve created a spreadsheet (cue either scary or optimistic music, depending on your perspective), and am looking forward to doing a little sorting of my own.
*I should note that if an applicant doesn’t match, then there is a second small match that used to be referred to as the Scramble, where applicants re-apply for program spots that have been left unfilled. This doesn’t happen often at Michigan, and certainly isn’t the best way to get the match of your dreams as the most desirable spots are already taken, but can yield an acceptable outcome for all involved.

